Renal cell carcinoma (RCC), generally referred to as Kidney Cancer, is among the ten most common cancers for men and women. The lifetime risk for developing RCC in men is about 1 in 46 and 1 in 80 for women. The American Cancer Society estimates about 79,000 new diagnoses and about 13,920 deaths from RCC in 2022 (American Cancer Society). In the UK, there were roughly 4,600 RCC-related deaths annually between 2016-2018. Furthermore, 13 people a day died of RCC in the UK during this period (Cancer Research UK). This article will delve into:
- The indication and effect of SABR on patients with RCC
- MVision’s guideline-based solution for your radiotherapy workflow

SABR for RCC
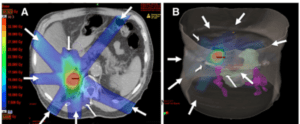
Stereotactic ablative radiotherapy (SABR), also known as stereotactic body radiation therapy (SBRT), is a highly focused form of radiation treatment. SABR gives an intense dose of radiation concentrated to a tumour while limiting the radiation to the surrounding organs. The number of treatment sessions is lower than standard radiotherapy. The beams are directed from different angles meeting at the tumour with high precision and accuracy. This lowers the risk of damage to the normal cells. Today, SABR has proved to be a safe and effective treatment for different cancer types (Memorial Sloan Kettering Cancer Center).
The treatment decision for RCC is dependent on many factors, including tumour type, the stage of the disease, patient health status, and therapy availability. For the localised disease of RCC, the primary treatment is surgery, sometimes followed by systemic therapy. For advanced, metastatic cases, systemic therapy is the first choice. However, the encouraging results of this highly conformal and effective radiotherapy technique open new directions for its implementation.
The National Comprehensive Cancer Network (NCCN) guidelines mention that SABR may be considered for selected patients with the (localised) disease for treating primary tumors. A pooled analysis of SABR for primary RCC reported individual patient data sets from 223 patients from 9 International Radio-surgery Oncology Consortium for Kidney institutions across Germany, Australia, the United States, Canada, and Japan. Among the findings, SABR was well tolerated and had an acceptable impact on renal function. The treatment was locally effective. At four years, the rates of local control, cancer-specific survival, and progression-free survival were 97.8%, 91.9%, and 65.4% (Siva, Shankar, et al.).
In case of a limited number of metastases at diagnosis or relapse, SABR is recommended as an alternative to metastasectomy or ablation techniques (National Comprehensive Cancer Network). A study of the GETUG group reported retrospective data of 188 RCC patients who received SABR with curative intent in 6 French referral centres, between 2008-2015. SBRT was performed for oligoprogressive disease, oligometastatic disease, or residual tumour after a partial response to systemic treatment. The study noted acute and late severe toxicities in 2.6% of the cases. The local control rate of metastases treated with SABR was 87.5% and 82.9% at 6- and 12-months. A quarter of oligometastatic patients did not relapse, and 40% did not need systemic treatment. In an oligoprogressive setting, the median time to progression was 8.6 months, and the time to administration of systemic therapy was 10.5 months (Meyer, Emmanuel, et al.)
A recent, prospective Phase II study shows that SBRT is beneficial in metastatic RCC recently reported similar results. A multi-centric Canadian trial used SABR for oligoprogression in Metastatic RCC Patients Receiving Tyrosine Kinase Inhibitor Therapy. The trial included 37 patients, reporting a 93% local control and a 92% overall survival after one year. The median time to change in systemic therapy was 12.6 months, and there were no grade 3 or higher radiotherapy-related toxicities (Cheung, Patrick, et al.)
Another Phase II trial from the USA enrolled 20 patients on first to fourth line systemic therapy with three or fewer sites of progression of RCC. The local control at 1 year was 100%. The median time from SABR to the onset of new systemic therapy or death was 11.1 months, and the median duration of SABR-aided systemic therapy was 24.4 months. Only one patient developed severe toxicity (Hannan, Raquibul, et al.).
Despite recent advances in systemic therapy, resistance can develop and new treatments can be costly. In the context of poor disease prognosis, any time gain is important, even if it is measured in months. RCC is considered a radio-resistant tumour, but delivering high doses per fraction may overcome this limitation. Increased accuracy and precision are required to deliver this kind of treatment safely,
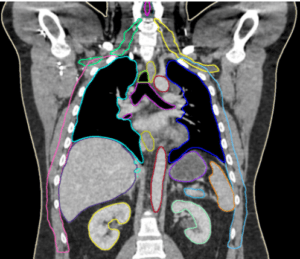
Standardising Guideline-Based Segmentation, GBS™, for your radiotherapy workflow.
MVision’s guideline-based segmentation system improves standardisation and increases consistency. Among its many features, the Advanced Abdomen & Thorax Model helps to avoid the organs-at-risk in treatment planning while handling both contrast and non-contrast CT scans.
MVision’s Guideline-Based SaaS Solution
MVision AI is the pioneer of guideline-based AI segmentation, GBAIS™, radiotherapy software. Our deep learning system helps you automate contouring, including lymph node levels, to streamline your cancer treatment planning. Our software complies with HIPAA, and GDPR, bringing the highest quality radiotherapy planning SaaS solution for your oncology department.
Book a demo to explore guideline-based segmentation for your clinic.
MVision AI is active on LinkedIn, Twitter, Facebook, and Instagram. Follow us on social media and subscribe to our newsletter to stay up-to-date on the latest MVision AI news.
Are you eager to learn more? We welcome you to contact MVision AI:
c/o Terkko Health Hub, Haartmaninkatu 4, 00290 Helsinki, Finland.
Tel: +358 (0) 40 5489 229
Email: info@mvision.ai
For media inquiries:
+358 40 500 7915; pr@mvision.ai
Sources
Cheung, Patrick, et al. “Stereotactic Radiotherapy for Oligoprogression in Metastatic Renal Cell Cancer Patients Receiving Tyrosine Kinase Inhibitor Therapy: A Phase 2 Prospective Multicenter Study.” European Urology, vol. 80, no. 6, 2021, pp. 693–700., https://doi.org/10.1016/j.eururo.2021.07.026.
Hannan, Raquibul, et al. “Phase II Trial of Stereotactic Ablative Radiation for Oligoprogressive Metastatic Kidney Cancer.” European Urology Oncology, 2022, https://doi.org/10.1016/j.euo.2021.12.001.
“Key Statistics about Kidney Cancer.” American Cancer Society, https://www.cancer.org/cancer/kidney-cancer/about/key-statistics.html.
“Kidney Cancer Statistics.” Cancer Research UK, 27 Jan. 2022, https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/kidney-cancer#heading-One.
Meyer, Emmanuel, et al. “Stereotactic Radiation Therapy in the Strategy of Treatment of Metastatic Renal Cell Carcinoma: A Study of the Getug Group.” European Journal of Cancer, vol. 98, 2018, pp. 38–47., https://doi.org/10.1016/j.ejca.2018.04.008.
National Comprehensive Cancer Network. https://www.nccn.org/professionals/physician_gls/pdf/kidney.pdf.
Siva, Shankar, et al. “Pooled Analysis of Stereotactic Ablative Radiotherapy for Primary Renal Cell Carcinoma: A Report from the International Radiosurgery Oncology Consortium for Kidney (IROCK).” Cancer, vol. 124, no. 5, 2017, pp. 934–942., https://doi.org/10.1002/cncr.31156.
“What Is SBRT?” Memorial Sloan Kettering Cancer Center, https://www.mskcc.org/cancer-care/diagnosis-treatment/cancer-treatments/radiation-therapy/what-sbrt#which-types-of-cancer-can-be-treated-using-sbrt-.


